
Day :
- Clinical Cardiology | Cardiovascular Research | Cardiac Diseases
Location: Madrid, Spain

Chair
Ersoz Gonca
Bulent Ecevit University, Turkey

Co-Chair
Marco Piciche
San Camillo-Forlanini Hospital, Rome
Session Introduction
Pablo Avanzas
Hospital Universitario Central de Asturias, Spain
Title: Activated macrophages and coronary artery disease: The role of neopterin and growth differentiation factor 15
Time : 11:00-11:30

Biography:
Dr. Avanzas graduated from Universidad de Navarra with full honours in 1998 and passed the Postgraduate Board in Cardiovascular Diseases at Gregorio Marañón Hospital in 2004. He took up a Spanish Heart Foundation Research Fellowship at Coronary Artery Research Unit, St. George´s Hospital Medical School in London and some months after that he was appointed as Associate Research Investigator of the Cardiovascular Biology Research Centre at St. George´s Hospital in London. He is Interventional Cardiologist at Hospital Universitario Central de Asturias in Oviedo, Spain, and author of more than 170 publications on peer reviewed journals. He was Associate Editor of “Revista Española de Cardiología” and member of several editorial boards.
Abstract:
Increasingly, cardiac biomarkers have provided important information in predicting short-term and long-term risk pro les in patients with acute coronary syndromes (ACS), particularly when they are used in combination. Among the numerous biomarkers, high-sensitivity C-reactive protein (hsCRP) has received widespread interest and a large database has been accumulated on their potential role as predictor of cardiovascular events. Macrophage activation, as shown by elevated levels of neopterin and GDF-15 (Growth diferentiation factor-15), has a key role in all phases of the atherothrombotic process. Neopterin is a pteridine that modulates intracellular redox state (NOS) and activates the expression of proinflammatory genes. Evidence gathered in recent years indicate that neopterin may be a useful tool in the assessment of cardiovascular risk in both apparently healthy subjects and patients with stable and unstable coronary artery disease. GDF-15 is one of more than 40 members of the transforming growth factor-𛽠superfamily and it was originally identified in activated macrophages. Accumulating evidence indicate that circulating levels of GDF-15 are associated with the risk of death and myocardial infarction, independent of clinical variables and other biomarkers, including hsCRP and cardiac troponins.
Mizanur Rahman
Karolinska Institute, Sweden
Title: HSP 60 as a T cell antigen activates peripheral blood and atherosclerotic plaque T-cells
Time : 11:30-12:00

Biography:
Mizanur Rahman has completed MSc in Biotechnology from The Royal Institue of Technology, Stockholm, Sweden and MSc in Molecular life science from Stockholm University, Stockholm, Sweden. At present he is a PhD student at Karolinska Institutet, Sweden. Since several years he is working on cardiovascular diseases and he has important findings on this area.
Abstract:
Cardiovascular diseases are defined as disorder or diseases of the heart and blood vessels. Atherosclerosis is one of major causes of cardiovascular disease development. Immune cells, including T-cells play an important role in the disease pathogenesis. Heat shock protein 60 (HSP 60) has been shown to be involved in cardiovascular diseases. This protein is expressed in response to heat or toxic effect to the cells, but elevated level of HSP 60 can be deleterious, including heart failure. However, antigenicity and immune response against HSP 60 are unclear.
Here, HSP 60 stimulated dendritic cells (DCs) were co-cultured with autologous peripheral blood T-cells. In addition, DCs generated from peripheral blood of atherosclerotic patients were also stimulated and co-cultured with atherosclerotic plaque T-cells. Further, HSP 60 stimulated DCs were co-culture with T-cell with or without anti-HLA II blocking antibodies. Immunophenotyping and cytokines profile was measured by flow cytometry and ELISA respectively.
We showed that HSP 60 induced DCs activation and Th1 cell activation through DCs, also induced inflammatory cytokines secretion, where the affect was inhibited by HLA-II blocking.
Studies suggest HSP60 as a co-stimulatory factor but our observation shows that HSP 60 is also a T cell antigen and it activates Th1 cells in atherosclerotic plaque.
Lingfang Zeng
King’s College London, UK
Title: HDAC7-derived 7-amino acid peptide functions as a phosphate group transfer
Time : 12:00-12:30

Biography:
Dr Lingfang Zeng has completed his PhD at the age of 27 years from Beijing Normal University, China. He is now a Senior Lecturer in the Cardiovascular Division, Faculty of Life Science and Medicine, King’s College London. He has published more than 40 papers in reputed journals and has been serving as an editorial board member of repute.
Abstract:
Histone deacetylase 7 (HDAC7) belongs to the class II HDAC family and plays a pivotal role in the maintenance of endothelium integrity. There are 8 splicing variants in mouse HDAC7 mRNAs. Within the 5’ terminal non-coding area of some variants, there exist some short open reading frames (sORFs). Whether these sORFs can be translated and whether the resulting peptides play roles in cellular physiology remain unclear. In this study, we demonstrated that one sORF encoding a 7-amino-acid (7-aa) peptide could be translated in vascular progenitor cells (VPCs). Importantly, this 7-aa peptide (7A) could transfer the phosphate group from the phosphorylated Ser393 site of MEKK1 to the Thr145 site of 14-3-3γ protein. The phosphorylated 7A (7Ap) could then directly phosphorylate 14-3-3γ protein in a cell-free, in-gel buffer system. In vitro functional analyses revealed that 7A and 7Ap increased VPC self-renewal and migration and enhanced vascular endothelial growth factor (VEGF)-induced VPC migration and differentiation toward the endothelial cell (EC) lineage, in which MEKK1 and 14-3-3γ served as the upstream kinase and the downstream effector, respectively. Knockdown of either MEKK1 or 14-3-3γ attenuated VEGF-induced VPC migration and differentiation. Exogenous 7Ap could rescue the effect of VEGF on the MEKK1 siRNA-transfected VPCs but not on the 14-3-3γ siRNA-transfected VPCs. In vivo studies revealed that 7A, especially 7Ap, induced capillary vessel formation in Matrigel plug assays, increased re-endothelialization and suppressed neointima formation in the femoral artery injury model, and promoted foot blood perfusion recovery in the hindlimb ischemia model by increasing Sca1+ cell niche formation. These results indicate that the sORFs within the non-coding area can be translated and that 7A may play an important role in cellular processes, such as proliferation, migration and differentiation, by acting as a phosphorylation carrier.
Sara Badia
Universitari Germans Trias i Pujol, Spain
Title: Perceval S and coronary artery bypass grafting, contradiction or full harmony?
Time : 12:30-13:00

Biography:
Sara Badia is a Cardiac Surgeon trained in Madrid, who completed her training visiting numerous important centers in USA like the Cleveland Clinic (under the direction of Dr. Sabik) or the Children´s National Medical Center in Washington D. C. (Dr. Jonas), and also in Europe like Allgemeines Krankenhaus (AKH) in Vienna (Prof Laufer, Prof Kocher), and off pump coronary artery bypass grafting (OPCABG) training in Leuven Belgium with Prof. Paul Sergeant.
She is a surgeon who loves improving and be updated in the latest techniques like minimally invasive aproaches and last generation valves. Actually, she is working in Barcelona, in one of the National hospitals where Perceval S bioprosthesis is usually used. This publication try to solve some doubts about the use of this prosthesis.
Abstract:
Background / Study Objective:Coronary artery disease is common in patients who undergo an aortic valve replacement.Concomitant coronary artery bypass grafting (CABG) procedure does not necessarily contradict with the use of last generation sutureless bioprosthesis, but, publications about this combined approach are very scarce.
The objective of this study is to describe the results of aortic valve replacement with Perceval S bioprosthesis with concomitant CABG in our Center.
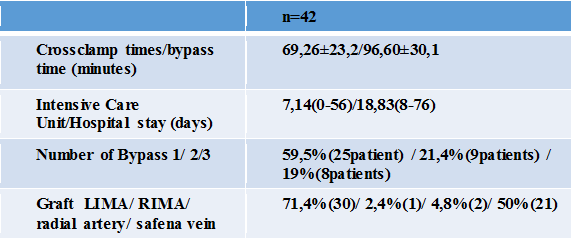
Methods: From our database we retrospectively described the outcomes of 42 patients who underwent aortic valve replacement with a last generation sutureless bioprosthesis (Perceval S) with CABG at the same procedure.It was used as graft: left internal mammary artery (LIMA), right internal mammary artery (RIMA), radial artery and safena vein.
From 1 to 3 arteries were revascularized per patient.
Mean age: 78,19±5,1. They were mostly man (women 35,7%).
Cardiovascular risk factors: Hipertension 97,6%; Diabetes 38,1%, obstructive pulmonary disease 21,4% of the patients.
Mean Logistic EuroScore II 10,73%.
Results. Table 1: Surgical Outcomes
Results. Table 2: Complications
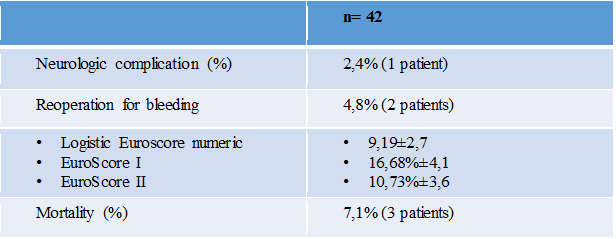
Conclusions: Excellent results were achieved in patients undergoing aortic valve replacement with Perceval S sutureless bioprosthesis and concomitant coronary artery bypass grafting. Although high aortotomy is needed for Perceval S implantation, is possible to perform CABG also with safena vein if necessary in a safely way.Perceval S is a feasible alternative for patients with aortic valve stenosis and coronary heart disease, shortening the crossclamp time, extracorporeal circulation time and comorbidities derived therefrom.
Ersoz Gonca
Bulent Ecevit University, Turkey
Title: A pharmacological study of a new spiro-cyclic benzopyran activator of the cardiac mitokatp channel on ischemia/reperfusion-induced ventricular arrhythmias
Time : 14:00-14:30

Biography:
Ersöz GONCA has completed his PhD in 2008 from Abant Ä°zzet Baysal University and postdoctoral studies from Robert Gordon University, the Institute of Health and Welfare Research in 2012. He is studying on ischemia/reperfusion-induced ventricular arrhythmias and myocardial injury. He has been conducting his researches in Bülent Ecevit University, Biology Department since 2009.
Abstract:
Background/Introduction:4ı-(N-(4-acetamidobenzyl))-2,2-dimethyl-2,3-dihydro-5ıH-spiro[chromene-4,2ı-[1,4]oxazinan]-5ı-one (compound A) was synthesized as a new spiro-cyclic benzopyran activator of the cardiac mitochondrial ATP-dependent potassium (mitoKATP) channels. A previous study showed the anti-ischemic properties of Compound A (1).
Purpose: This study was performed to research the effect compound A on ischemia/reperfusion (I/R)-induced ventricular arrhythmias. In our previous study, we suggest that both mitoKATP channel activation and sarcolemmal ATP-dependent potassium (sarcKATP) channel inhibition confer protection against I/R-induced arrhythmias (2); therefore, we also aimed to test the hypothesis that a combination of mitoKATP channel activation and sarcKATP channel inhibition may be even more effective at decreasing ventricular arrhythmias.
Methods: We performed myocardial I/R by ligating the left main coronary artery for 6 minutes followed by loosening the bond at the coronary artery for 6 minutes in anesthetized rats. The experimental groups were as follows: (1) Vehicle control, (2) Compound A (3 mg/kg) (3) Compound A (10 mg/kg.) (4) Diazoxide (5) HMR 1098 (6) Compound A (10 mg/kg)+HMR 1098, and (7) Diazoxide+HMR 1098 group.
Results: Compoud A at a dose of 10 mg/kg decreased both the arrhythmia score and the total length of arrhythmias (P<0.01). Diazoxide at a dose of 40 mg/kg, a selective mitoKATP channel opener as a reference drug only decreased the total length of arrhythmias (P<0.01). Compound A at a dose of 10 mg/kg was more effective at decreasing the duration of arrhythmias than a dose of 3 mg/kg of compound A and diazoxide. The combination of both diazoxide and compound A with HMR 1098, a selective sarcKATP channel blocker, did not exhibit any additive or synergic effect on the antiarrhythmic effect of each drug alone.
Conclusion (s): These results reveal that compound A may have a dose-dependent antiarrythmic effect, which is more pronounced than the antiarrhythmic effect of diazoxide. Both mitoKATP channel activation and sarcKATP channel inhibition at the same time may not reveal any additive antiarrhythmic effect on I/R-induced arrhythmias.
Ryan D. Andal
Makati Medical Center, Philippines
Title: Subclavian artery stenosis/thrombosis in a post CABG patient while undergoing dialysis for CKD using Left AV fistula, presenting as ST elevation MI and acute limb ischemia
Time : 14:30-15:00

Biography:
Ryan D. Andal has completed his College at the age of 18 years from De La Salle University Manila with a degree in Medical Physics and postdoctoral studies from University of Santo Tomas , Manila. He trained in internal medicine at the Makati Medical Center and his 3rd year of fellowship in cardiology. He is board certified in Internal Medicine and plans to pursue interventional cardiology after his fellowship training.
Abstract:
Coronary subclavian steal syndrome is a rare disorder, mostly unrecognized and underdiagnosed , seen in patients developing subclavian artery (SA) stenosis after Coronary Artery Bypass Graft (CABG) using the LIMA –LAD graft diverting blood flow from the native coronary LAD back to the graft LIMA –LAD into the subclavian artery in a retrograde fashion. This is also the same for the vertebral artery where blood is diverted back from the brain into the subclavian artery.
This disorder causes significant symptoms which is brought about by ischemia coming from the heart, left upper extremity and the brain . It is a catastrophic event where only very few case reports have been described and reported .Moreover, it has been also described that a coronary steal from a LIMA graft post CABG can present as angina while undergoing hemodialysis. This phenomenon is documented through cardiac catheterization with evidence blood flow steal from the internal mammary artery graft while on dialysis, without subclavian subclavian artery stenosis.
This is a case report of a patient with coronary-subclavian steal syndrome caused by a proximal subclavian artery stenosis in a post CABG patient with a LIMA-LAD graft aggravated by ongoing dialysis using AV fistula on the left arm. A combination f 2 phenomena that can lead to detrimental outcome if not treated appropriately though revascularization.
Rajeev Agarwala
Jaswant Rai Speciality Hospital, India
Title: 25 years of statin/ view from the hill top
Time : 15:00-15:30

Biography:
Dr. Rajeev Agarwala is DM Cardiology from GB pant Hospital New Delhi india 1990 and chairs the department of cardiology at Jaswant Rai Speciality Hospital Meerut. He is an active clinician with bulk experience in invasive cardiology. He holds the Limca book of record for India for implanting free pacemaker. He has published more than 20 papers and review articles in various journals and actively pursues vascular biology and statinology.
Abstract:
This is a review kind of presentation featuring evolution of statins usage form total cholesterol reduction to LDL reduction Hypothesis. Its documented effects in reducing cardiovascular mortality. It rationalizes European view of chasing LDL numbers rather than high blanket dose of statin, an american view. It also emphasizes death of HDL manipulation era and why it failed. Pleiotropic effects are also questionable. The talk will position ezetimibe and PCSK9 in current medical practices and will also feature legacy effects of statin and progressive calcification with its usage. The presentation ends with inspiration from existing guidelines. The talk will be of immense use to clinician.
Nadeeja Himanthi Gamalath Seneviratne
The National Hospital of Sri Lanka, Sri Lanka
Title: Factors associated with survival of post Coronary Artery Bypass Graft (CABG) patients registered in cardiology Unit, National Hospital Sri Lanka (NHSL)
Time : 15:30-16:00

Biography:
Dr. (Mrs) NHG Seneviratne, MBBS (Sri Lanka), MD Medicine (Colombo). – She obtained MD Medicine from Post Graduate Institute of Medicine, University of Colombo in 2013. Currently she is undergoing post doctoral training in Cardiology at Institute of Cardiology NHSL. She has published four papers in local forums and one poster presentation which won the gold medal for best poster in 2010. She has done oral and poster case presentations at Asian Interventional Cardiovascular Therapeutices Congress 2015, Dhaka, Bangladesh. She works as a sub inspector in ODYSSEY and TRIUMPH multi centre clinical trails and a resource person in frailty study.
Abstract:
CABG is one of the treatment options for the patients with coronary artery disease (CAD). This study was aimed to describe survival up to occurrence of cardiac events and factors associated with them among CABG patients at NHSL.
Retrospective analytical study was carried out among the patients who had undergone CABG at least one year before the date of data collection. Cardiac event was defined as new occurrence of any condition namely; unstable angina (UA), ST elevated myocardial infarction (STEMI), non ST elevated myocardial infarction (NSTEMI) and heart failure (HF). Survival was assessed up to the defined cardiac events.
The sample (n=421) consists 74.6% males and mean age was 63.16years (SD = 7.86). Event rates were UA (13.3%), STEMI (0.5%), NSTEMI (3.1%) and heart failure (8.6%). Kaplan-Mayer survival analysis revealed the probability of survival at 5 years was 79.6% (CI 0.781-0.871) and 10 year was 58.1% (CI 0.516- 0.688). Cox regression revealed significant associations with age (HR- 0.973, p=0.023), family history (FH) of hypertension (HR-2.2, p=0.044) compared to negative family history and activities of daily living (ADL) independency (HR=0.16, p= 0.011) compared to the ADL dependency.
CABG surgery reserves its own place in management of CAD. Sri Lankan survival data of CABG patients seems to be similar to other countries of the world. Age, status of ADL prior to CABG and family history of hypertension were significantly associated with survival.
Ersoz Gonca
Bulent Ecevit University, Turkey
Title: The effect of cannabidiol on ischemia/reperfusion-induced ventricular arrhythmias: The role of adenosine A1 receptors
Time : 16:15-16:45

Biography:
Ersoz Gonca has completed his PhD in 2008 from Abant Ä°zzet Baysal University and postdoctoral studies from Robert Gordon University, the Institute of Health and Welfare Research in 2012. He is studying on ischemia/reperfusion-induced ventricular arrhythmias and myocardial injury. He has been conducting his researches in Bülent Ecevit University, Biology Department since 2009.
Abstract:
Backgroud/Introduction: Cannabidiol (CBD) is a nonpsychoactive phytocannabinoid with anti-inflammatory activity mediated by enhancing adenosine signaling [1,2]. As the adenosine A1 receptor activation confers protection against ischemia reperfusion (I/R)-induced ventricular arrhythmias, we hypothesized that CBD may have anti-arrhythmic effect through the activation of adenosine A1 receptor.
Purpose: We aimed to research the effect of CBD on the incidence and the duration of ischemia reperfusion (I/R)-induced ventricular arrhythmias, and to investigate the role of adenosine A1 receptor activation in the possible antiarrhythmic effect of CBD.
Methods: Myocardial ischemia and reperfusion were induced in anesthetized male rats by ligating the left anterior descending coronary artery for 6 minutes and by loosening the bond at the coronary artery, respectively. CBD alone was given in a dose of 50µg/kg, 10 minutes prior to coronary artery occlusion and co-administrated with adenosine A1 receptor antagonist 8–Cyclopentyl-1,3-dipropylxanthine (DPCPX) in a dose of 100µg/kg, 15 min prior to coronary artery occlusion to investigate whether the antiarrhythmic effect of CBD is modified by the activation of adenosine A1 receptors. The experimental groups were as follows (1) vehicle control (n = 10), (2) CBD (n= 9), (3) DPCPX (n= 7), and (4) CBD+ DPCPX group (n = 7).
Results: CBD treatment significantly decreased the incidence and the duration of ventricular tachycardia (VT), total length of arrhythmias and the arrhythmia scores compared to control during the reperfusion period. DPCPX treatment alone did not affect the incidence and the duration of any type arrhythmias. However, DPCPX aborted the antiarrhythmic effect of CBD when it was combined with it. Any drug treatments affect neither QT nor QRS intervals prior to and during the ischemic period.
Conclusion (s): The present results demonstrate that CBD has an antiarrhythmic effect against I/R-induced arrhythmias and the antiarrhythmic effect of CBD may be mediated through the activation of adenosine A1 receptor. The underlying mechanism of the antiarrhythmic effect of CBD may not depend on its direct electrophysiological effect. The present results support the notion that endogenously released adenosine does not significantly affect the occurrence of ventricular arrhythmias via the activation of adenosine A1 receptor.
Hariharan Munganda
Asian Institute of Medical Sciences, India
Title: Correlation between serum homocysteine levels and serum vitamin b12 levels in first time acute mi patients with relative lack of conventional risk factors in (rural) north Indian population
Time : 16:45-17:15

Biography:
Hariharan is doing DNB postgraduation in internal medicine and research in nephrology, cardilogy, infectious diseases and diabetology. He has published papers in national and international journals and attended various conferences for oral and poster presentations.
Abstract:
Introduction: Indian patients have higher incidence of cardiac diseases inspite of the conventional risk factors comparable to western counterpart.The increased excess cardiac risk in Indians as compared to western population remains unexplained. Low serum vitamin B 12 and high serum homocysteine levels are known predictors of cardiovascular mortality and are highly frequent in Indians . Our present study was taken to ascertain whether these two factors are responsible for excess cardiac risk in indians.
Aim of the study : We in our study aimed to study subjects with AMI in whom most of the known risk factors for cardiovascular disease are absent but were deficient in vitamin B12 or having high S. homocysteine levels and correlate the two parameters.
Material and Methods: Subjects presenting to our Asian tertiary care hospital who were having first time MI(naive)patients without any cardiac disease or any treatment and without any family history .All patients with STEMI less than 12hours of duration and no past history of cardiac disease/DM/HTN/Dyslipidemia were included.After obtaining written informed consent ,detailed history was sought and subjects were again evaluated for routine laboratory biochemical parameters including Serum vitamin B12 levels and serum homocysteine levels, coronary angiography and ECHO. 100 Subjects who were found to be suffering from AMI were included as cases , and 20 subjects showing symptoms of chest pain but lacking any elevation in CK total or CK MB , no changes on ECG and normal ECHO and angiographic findings were included as controls.
Results: Various risk factors of AMI including Age, non vegetarian diet, DM, HTN, Family history, BMI, Dyslipidemia, Low HDL, High TG, LDL, Cholesterol were found to be lower in cases compared to controls. Serum vitamin B 12 levels were found to be significantly lower(<0.0001) and serum homocysteine levels(<0.0001) were significantly higher in cases. Further Weak downhill (r=-0.367) but significant correlation was noted between S. Vit B 12 and S. Homocystein levels. Also significant association was noted between low s. Vit. B12 and high homocysteine and Acute MI. ROC curve was plotted to evaluate predictive value of parameters for AMI. Vitamin B12 was found to have AUC of 96.2 % and sensitivity of 95% and specificity of 100 % at cut off value lower than 360 pg/L. Also Serum homocysteine was found to have AUC of 93.2 % and sensitivity of 86% and specificity of 100 % at cut off value higher than 25.3 mcg/L.
Conclusion: In individuals especially younger age group(20-30years) who lack conventional risk factors/family history of coronary artery disease, low serum vitamin B12 levels and high serum homocysteine levels pose significant risk of heart disease. Serum vitamin B12 and serum homocysteine levels should be regularly assessed to predict the risk of AMI in subjects with lack of other risk factors along with dietary and lifestyle changes.
Riccardo Turri
Mirano General Hospital, Italy
Title: Multi-district atherosclerotic disease: Mid-term outcome of hybrid or totally endovascular coronary and carotid revascularization
Time : 17:15-17:45

Biography:
Riccardo Turri graduated with the best ratings at Padua University in Italy; he was always engaged in studying and applying into invasive cardiology and acute cardiologic care. His competences include coronary angioplasty, bifurcation lesions, coronary imaging and functional assessment, limb and BTK angioplasty. In the last 3 years, he worked as an interventional cardiologist at Mirano General Hospital, near Venice, Italy.
Abstract:
Background: The socio-economic impact of multi-district atherosclerotic disease is elevated for frequent hospitalizations and morbidity/mortality.
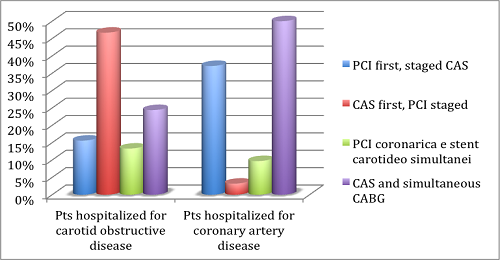
Aim: Assess clinical characteristics, angiographic findings, therapeutic strategy and outcome of patients hospitalized with a concomitant diagnosis of coronary artery and carotid obstructive diseases.
Methods: We evaluated all patients hospitalized from 2006 to 2012. Revascularization strategies were hybrid (carotid stenting CAS and cardiac surgery CABG) or totally endovascular (coronary angioplasty PCI and CAS).
Results: 107 patients were enrolled, 42.1% were hospitalized for carotid obstructive disease (groupA), and 57.9% for coronary artery disease (groupB). Patients were treated with PCI and staged CAS in 28% of cases (15.6% in groupA, 37.1% in groupB), with CAS and staged PCI in 21.5% of cases (46.7% in groupA, 3.2% in groupB), with CAS and simultaneous CABG in 39.3% of cases (24.4% in groupA, 50% in groupB) and with PCI and simultaneous CAS in 11.2% of cases (13.3% in groupA, 9.7% in groupB). 30-days results: Mortality 0%, major/minor stroke 3.7% (2.2% in groupA, 4.8% in groupB), myocardial infarction 2.8% (0% in groupA, 4.8% in groupB), major bleeding 5.6% (2.2% in groupA, 8.1% in groupB). Major bleeding affected only patients with acute symptoms and 11.9% of patients following CABG. Follow-up results: Cardiovascular mortality 4.7% (2.2% in groupA, 6.5% in groupB), all-cause mortality 2.8% (4.4% in groupA, 1.6% in groupB), stroke 0.9% (2.2% in groupA, 0% in groupB), myocardial infarction 2.8% (4.4% in groupA, 1.6% in groupB). The only predictor of mortality at follow-up was the in-hospital stroke (HR 7.6 for all-cause mortality, 16.5 for cardiovascular mortality).
Conclusions: Patients with concomitant coronary artery disease and carotid obstructive disease were treated with a high procedural success, following a hybrid or totally endovascular revascularization. Patients hospitalized in an acute setting have more strokes and bleedings at 30 days; these patients need therefore most careful assessment and treatment.
Image
Yanal F Al-Naser
Queen Alia Heart Institute, Jordan
Title: 35 years off warfarin-Standing the “Test “or “Challenge†of time?
Biography:
Yanal Al-Naser is a consultant cardiac surgeon from Amman-Jordan. He graduated from University of Jordan in 1999 and was awarded the Jordanian boards in general surgery (2004) and cardiac surgery (2009). He was trained in Manchester –England as an adult cardiac surgeon and finished his training in 2012. He became a consultant adult cardiac surgeon in 2012 at Queen Alia Heart Institute in Jordan. He has a number of publications, and is a member of the Jordanian Cardiac society and the Royal College of Surgeons in the UK.
Abstract:
A 46 year old female patient, with no medical illnesses was referred to my clinic with effort intolerance and palpitations of four years duration. Her history dates back to when she was 11 when she had an Aortic and Mitral valve replacement due to rheumatic causes, she had a size 19mm bileaflet mechanical aortic valve and a size 27mm bileaflet mechanical mitral valve. She was started on warfarin and took it for three months of her life as documented by her family members and follow up notes till she decided to stop it. She stated that she took no medications at all and was completely asymptomatic, she got married and had three children, all a normal vaginal delivery aided by a mid wife at home. Her 2DECHO showed a grade three para-leaking aortic and mitral valves, and was referred to me for a redo AVR and MVR 35 years later, being off warfarin for all that period and was asymptomatic for 30 years and never had a stuck valve. Her coagulation profile was normal, with an INR of 1, I operated on her and found a rim of pannus surrounding the valves, but the leaflets were mobile. I replaced both valves using St Jude size 21 Aortic Valve and size 29 Mitral valves, both mechanical. There are a few cases described in literature about mechanical valves with no warfarin, but I believe this is one of those with the longest –off warfarin- history.
Biography:
Doug is a cardiac sonographer of 18 years. Working pain free as a result of doing ‘movment training’.
Mark is a world leader in body strength and condition and ‘movement training’.They educate sonographers all over the world to live and work pain free.
Abstract:
Statement of the Problem: Worldwide sonographers of all modalities suffer an epidemic, up to 90%, on-the -job pain/injury rate. 30% of those folks become debilitated and become disabled or forced to make a career change. The purpose of this presentation will demonstrate to sonographers correct exercise/stretching technique using proper movement patterns. Optimized movement patterns as related to the body and the type of work, ultimately decrease injury and give you the ability to work pain free. Methodology: Discussion on how work induced sonographer pain/injury occurs. What are the biomechanics of pain/injury. Demonstration of proper corrective exercises choice and technique to increase career longevity. ‘Corrective’ exercise, is not the same as ‘fitness’ exercise. Corrective exercise and a gym workout are dissimilar. The differences and similarities explained. Correct movement patterns lead to dramatically reduced injury and career longevity. Demonstration on corrective Training Principles and Techniques. Training Protocols Corrective exercises for problem areas: Shoulders/Neck, Arms/Wrist, Lower Back, Hips, Legs, Focus on areas for corrective movement. How to implement a corrective program into your routine. Simple stretches and exercises that can be done anywhere. Findings: ‘Corrective Movement’ stretching and exercise allows the body to be trained to withstand the rigors of what you ask it to do. Conclusion: Sonographers worldwide suffer from an epidemic rate of on-the-job pain/injury. There are practical, implementable solutions to allow a sonographer to continue doing their job for years to come. ‘Movement Training’ combined with proper ergonomics is the solution.
Maria Korre
Harvard T.H. Chan School of Public Health, USA
Title: Effect of body mass index on left ventricular mass in career male firefighters

Biography:
Abstract:
David Rosenberg
University of los Andes, Santiago, Chile
Title: Topical application of statins for controlling periodontal immune responses: a revolution in periodontal disease prevention and treatment?

Biography:
David graduated in 1991 from the Faculty of Dentistry at the University of Chile. From 1992 to 1995 he pursued a Masters of Science in Periodontology and Osseointegration at the Catholic University of Leuven (KUL Leuven, Belgium), under the guidance of professors Daniel van Steeberghe and Marc Quirynen. Upon returning to Chile, Dr. Rosenberg founded the International Center of Periodontology and Osseointegration (CIPO). A successful private practice, considered one of the most important in Santiago de Chile. He is an active member of the European Association of Osseointegration since 1993, and the Academy of Osseointegration since 2000. He is also an Associate Professor and Researcher at the University of the Andes, since 2001. From the years 2006 to 2009 he pursued Oral and Maxillofacial Surgery training with Professor Bertrand Jaques at CHUV University Hospital in Lausanne, Switzerland. Since 2009, David serves as the Director of Graduate Studies of the Faculty of Dentistry and part of the academic staff of Department of Oral and Maxillofacial Surgery at the University of the Andes. In 2011, he enrolled in the PhD program at the International University of Catalunya, researching topics in the areas of Periodontology and Oral Medicine. In February 2015, he was appointed as the Chief of Dentistry at the University Hospital of the Universidad de los Andes. It is noteworthy that in the last 5 years, David was awarded 2 important and large operating grants from the Chilean government, for Research and Development in the field of Dentistry and particularly in Periodontology. Dr. Rosenberg is an established lecturer and well-published in International journals, such as Journal of Periodontology and Journal of Clinical Periodontology, to list a few.
Abstract:
Periodontal disease (PD) is an inflammatory-infectious and destructive disease of the tissues surrounding teeth. Despite scientific and clinical advances worldwide, at least 90% of the adult population continues to suffer loss of periodontal tissues and eventually dentition, thereby deteriorating quality of life and generating enormous spending on oral as well as general health of the population. While the Biofilm is considered the main etiological factor of PD, it is now known that the immune system plays a key role in pathogenesis; responsible for the majority of the tissue destruction. Indeed, bacterial antigens do trigger an immuno-pathological reaction, which determines the susceptibility of the patient to the final outcome of the process. Furthermore, while the reversible lesion; gingivitis; under certain immunological conditions (yet unknown), can progress to a more complex, irreversible and destructive condition; periodontitis, this does not seem to depend solely on the type and amount of bacteria present, yet on a dysfunctional immune response, that in turn determines the pre-disposition of the patient to tissue destruction. Hence, tackling such pathologies solely via a bacteriological approach is deemed insufficient for a well-established clinical diagnosis, prognosis and efficacious preventive and therapeutic strategies. In this lecture, we will present scientific evidence supporting the application and potential of statins in clinical Periodontology. Predominantly indicated for dyslipidemia, statins possess extra-lipid properties and immuno-modulatory effects that favor their use for cardiovascular diseases (CVD). Given that CVD and PD share common paths in their physiopathology, our research group developed a statin-medicated toothpaste formulation and conducted a double-blinded controlled clinical trial, where the clinical efficacy (as an adjunct to conventional, periodontal treatment) was proven. Hence, the purpose of this presentation is to join forces with International University Research Centers and the pharmaceutical industry to develop a new generation of oral care products medicated with statins in order to impact the periodontal health indices of our patients and populations. It is an open invitation to fellow clinicians and researchers to be at the forefront of preventive and therapeutic periodontics; a revolution, perhaps one of the most significant in decades.
Imran Tahir
Worcestershire Acute Hospitals NHS, UK
Title: Can use of high sensitivity troponin (0 & 2 hrs) avoid unnecessary hospital admissions and save money?
Biography:
Dr Imran Tahir completed his MBBS from National University of Science and Technology at the age of 23 years. Currently training in medicine in West Midlands United Kingdom.
Abstract:
Background: Every four minutes someone is admitted to hospital suffering from a heart attack or a chest pain event in the UK, totalling over 150,000 hospitalisations a year. Chest pain is one of the most common presentations in the emergency department and quite a few of them get admitted as low risk ACS patients. With the developments in technology, we have increasingly sensitive troponin assays available. Previous-generation troponin assays have been used as diagnostic and prognostic markers in acute coronary syndrome patients and for risk stratification to guide triage decisions and aid in treatment selection. New, high-sensitivity troponin assays represent an important advance with added sensitivity for cardiac myocyte necrosis. High-sensitivity troponin assays detect concentrations of the same proteins that conventional sensitivity assays are aimed at detecting, just in much lower concentrations.
Objective: Can high sensitivity troponin avoid unnecessary admission and save money.
Method: We did the retrospective data analysis for 100 patients presenting in the emergency department of University hospitals Birmingham in the month of March 2016. All adult patients admitted with the diagnosis of ACS were included in the study.
Results: We included 100 patients admitted with the diagnosis of ACS under the medical team in the month of March 2016. 86% patients had a serial troponin done during the admission. Rest of the 14% had a single troponin done. Only 8% patients had a raise in the serial troponin, rest of them were discharged home. The average length of stay was 33 hours.
Discussion : Based on the results of this data analysis, it has been highlighted that considering the use of high sensitivity troponins at 0 and 2 hours coupled with appropriate risk stratification of patients presenting with chest pain in the Emergency department, can possibly help in safely discharging a major percentage of patients and avoiding unnecessary admissions to the hospital. At the same time making it possible to achieve the above objectives within the NHS policy of 4 hours breech time for the Emergency department
Conclusion: We have 5-10 patients every day presenting to the emergency department with chest pain. About 50% of them get admitted with the diagnosis of ACS. 86% of our patients could have been potentially discharged home by using high sensitivity troponin at 0 and 2 hours and hence could have avoided 86% admissions. This in turn could have saved quite some money. With the growing pressure in the emergency departments due to ever increasing number of patients all these high sensitivity tests could potentially make some difference.
Fawaz Almutairi
Security Force Hospital, KSA
Title: Difficult TAVI case with Coronary occlusion and literature review of coronary occlusion during TAVI
Biography:
To be updated soon...
Abstract:
75 year old male with multiple medical problem, had severe aortic stenosis, up on work up for TAVI we discover that he do have small annulus and low left main take off which make the case difficult for Medtronic Valve, we planned to do Edward valve with low implantation also for more accurate I did aortogram during valvuloplasty, left main was patent but surprisingly post valvuloplasty he develop 4+ aortic regurgitation and ST elevation, another aortogram confirm the presence of MID RCA 100% stenosis. The plan was to go after the valve which was deployed successfully then RCA was intubated with JR4, Export catheter showed presence of big thrombus in spite of ACT 230, the valve was seated appropriately and the RCA was TIMI III.
Withma Muthukumara
Lancaster Medical School, UK
Title: Case-based evaluation of the effectiveness of pci and CABG in the management of multi-vessel coronary artery disease
Biography:
To be updated soon...
Abstract:
Introduction: Multi-vessel coronary artery disease (CAD) can give rise to numerous disabling symptoms such as angina, shortness of breath (SOB) and fatigue, considerably impairing quality of life (QoL). Percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) have been developed to overcome these and increase life expectancy. The controversy over treatment preference has been a historical battle which CABG has dominated. However, the development of drug eluting stents (DES) is reducing the margin of difference in symptom improvement between the two interventions, making decisions difficult. Large randomised control trials (RCTs) such as SYNTAX, ARTSI/II and FREEDOM have set out to investigate the outcomes for each treatment and provide recommendations.
Aims: To measure QoL in terms of the symptom experience between 4 patients who had PCI/CABG and recognise the intervention providing the largest relief of symptoms. Additionally, explore the evidence behind PCI and CABG for multi-vessel CAD from RCTs and compare their outcomes with Case findings.
Method: 4 clinical cases, 2 undergoing PCI and 2 undergoing CABG, with multi-vessel CAD were selected. QoL was assessed using the Cardiovascular Limitations And Symptoms Profile (CLASP) questionnaire to explore the severity of symptoms before and after the intervention.
Results: Patients in the PCI group had an overall symptom reduction of 57.9% compared to only 38.9% in the CABG group. The greatest effect was seen in the angina category for PCI and SOB category for CABG, which resulted in a 100% relief of symptoms.
Conclusion: All patients had an improvement in symptoms to some degree, regardless of the type of intervention, but PCI patients had better outcomes across 4 more categories than CABG patients. RCTs report greater relief of symptoms following CABG, which was inconsistent with Case findings. CABG has demonstrated an increase in life expectancy and QoL in patients with SYNTAX scores ≥23 and more severe multi-vessel CAD, especially in diabetic patients, making it the treatment of choice.

Biography:
She has completed her Medical degree (Professional Doctorate) at the age of 26 years from Guilan University of Medical Sciences. She has 5 published and 3 under publish articles. She is the reviewer of the Journal of Biology and Today`s World (An International Biomedical Journal).
Abstract:
Background: Nowadays, percutaneous coronary intervention (PCI) is the most commonly used nonsurgical procedure which restores blood flow to the heart tissue. Such procedures may stimulate myocardial injury and release of myocardial necrosis biomarkers. Although higher levels of cardiac troponins (cTns) are associated with later adverse events, the prognostic importance of the lower levels of cTns, especially highly sensitive assays, is still a matter of controversy.
According to the above points, in the present study, we aimed to assess the prognostic power of mild to moderate elevations in hs-cTnT levels (as an indicator of periprocedural myocardial necrosis) for predicting the one-year outcome of PCI.
Methods and Results: In the present study, all the patients undergoing elective PCI between March 2011 and April 2013 at Tehran Heart Center were followed up. Based on our inclusion and exclusion criteria, finally, 2309 patients were qualified for the study. For measuring hs-cTnT, three blood samples were drawn: the first immediately before the beginning of PCI (baseline), the second 6 h after PCI, and the last 12 h after PCI. The hs-cTnT levels were analyzed using Elecsys 2010 analyzer and major adverse cardiac events (MACE) were assessed one month and one year after the procedure. Based on the pre- and post-procedural hs-cTnT levels, the patients were divided into three groups. But, the differences between the three hs-cTnT groups in terms of frequencies of MACE were not significant.
Conclusions: This prospective study demonstrated no association between mild to moderate elevations in hs-cTnT after PCI and one-year MACE.
- Interventional Cardiology | Coronary Heart Diseases | Cardiac Surgery
Location: Madrid, Spain

Chair
Hatem AlMasri
King Abdulaziz Medical City, Saudi Arabia
Session Introduction
Hatem AlMasri
King Abdulaziz Medical City, Saudi Arabia
Title: Correction using surgical procedure of tetralogy of fallot with small pulmonary annulus – Can we preserve the valve annulus
Time : 09:30-10:00

Biography:
Dr. Hatem Al-Masri is a cardiac critical care intensivist and consultant of cardiac surgery. Dr. Al-Masri completed his medical degree (M.D.-Doktorate(PhD) at Charles University – Faculty of Medicine, holds a degree in biochemistry from the University of Waterloo - Canada, completed his residency training in Germany (Leading Facharzt) and holds training fellowships in Cardiac Surgery from IJN, KL, Malaysia, Switzerland, and Canada. Dr. Al-Masri is the author of an award-wining medical research paper titled “Hemodynamic Support Requires Integrated Approach Comparing LVAD vs. IABP in Patients Experiencing Left Venticular Failure” (Best Paper of Young Cardiac Surgeon) at the 8th International Congress of Update in Cardiology and Cardiovascular Surgery (UCCVS 2012) awarded by European Society for Cardiovascular Surgery, World Society of Arrhythmias (WSA ) and the Society of Cardiology and the International Academic of Vascular and Endovascular Surgery (ISCP). Dr. Al-Masri is a member of the Medical German Association, Malaysian Medical Association and the Saudi Medical Council.
Abstract:
To determine the outcome of repair of Tetralogy of Fallot (TOF) with small pulmonary annulus by preserving the pulmonary valve.
All consecutive patients (n=41) operated by a single surgeon using the above technique were reviewed. The pulmonary annular size was based on preoperative transthoracic or intraoperative TEE measurement. All patients had pulmonary annular size with Z value of -2 or less.The mean age of the patients were 6.2 years (range from 2 to 23). There were more males to females (26:15). All patients were cyanosed, and 11 were severely cyanosed. Eleven patients had previous Blalock-Taussig shunts, with 2 patients had 2 shunts done. The mean Z score of the pulmonary valve annulus was Z – 4.3 +/- 1.69 mm. All patients had bicuspid and/or dysplastic pulmonary valve. All except 4 patients had infundibular and pulmonary artery augmentation. Post correction mean RV/LV pressure ratio was 0.83. The mean pulmonary valve gradient was 34.8 mmHg. The mean cardiopulmonary bypass time was 143 min and the mean cross-clamp time was 77 min. The mean extubation time was 27 hours and mean ICU stay was 48 hours. All except 4 patients had either none or mild pulmonary regurgitation. There was only 1 mortality in this series. Serial echocardiography was done on follow up. The longest follow up is 3 years and all patients who survive are currently doing well.
The preservation of the pulmonary valve in
Peter P. Karpawich
Wayne State University, USA
Title: When the guidelines don't apply: Contractility (dp/dt-max)-guided resynchronization pacing among patients with congenital heart and heart failure
Time : 10:00-10:30

Biography:
Dr Karpawich completed his Masters in Science degree from The University of Detroit and his Medical Degree from Hahnemann/Drexel University in Philadelphia, PA. His postdoctoral Residency in Pediatrics at The Children's Medical Center, University of Texas (Dallas), and Pediatric Cardiology Fellowship at Texas Children's Hospital, Baylor University (Houston). He founded and is Director of the Cardiac Electrophysiology Program at the Children's Hospital of Michigan and Professor of Pediatric Medicine, Wayne State University School of Medicine (Detroit). He has published over 200 scientific papers, textbook chapters and textbooks typically in the field of cardiac electrophysiology, pacing and heart failure management both in children and adults with congenital heart disease, and is on the editorial staff of several internationally-recognized medical journals.
Abstract:
Objectives: Patients (pts) with repaired congenital heart disease (CHD) can later develop heart failure (HF), leading to heart transplant (HT). Although cardiac resynchronization pacing therapy (CRT) has been applied to pts with normal anatomy, there is little information on CRT and CHD. This study evaluated acute hemodynamic contractility (dP/dt), not guidelines, among CHD pts to determine if it can predict chronic CRT efficacy.
Methods: Forty pts with CHD and HF (NYHA II-IV) underwent cardiac catheterization (cath) with dP/dt-max both before and after acute CRT pacing. If acute paced-dP/dt-max improved ≥ 15% from baseline with CRT pacing, pts were given the option of CRT. Clinical follow-up after CRT testing was from 2-144 months (mean 35).
Results: Preexisting pacemakers were present in 70% of pts. CHD was variable with 16/40 (40%) pts having either a single or systemic “right” ventricle morphology. Of the 40 pts, 26 (mean age 22y) met criteria for CRT benefit while 14 (mean age 29y) did not. There were no differences in age, QRS duration, left ventricular (LV) ejection fraction, LV end diastolic diameter, V contractility (dP/dt-max), nor PM between CRT groups. Among the CRT recipients, 21 pts (81%) improved in NYHA class and were removed from HT consideration. All underwent a repeat cath 6-14 months later showing continued improved contractility.
Conclusion: Since published CRT guidelines do not apply to CHD pts, a better way to select which CHD pts may benefit from CRT is needed. Pre-CRT testing by direct paced-contractility response improve patient selection and responder rates.
Ygal Plakht
Ben-Gurion University, Israel
Title: Acute MyoK+ardial Infarction: The association of changes in K+ levels and in-hospital mortality of patients with acute myocardial infarction
Time : 10:45-11:15
Biography:
To be updated soon...
Abstract:
Background: Serum potassium levels (K, mEq/L) of patients with acute myocardial infarction (AMI) were found to be associated with short- and long-term outcomes. Nevertheless, significant fluctuations in K have been reported during the acute phase of an AMI.
Aims: To evaluate the association between K changes during the hospitalization and in-hospital mortality of patients admitted with AMI.
Methods: AMI patients hospitalized in a tertiary medical center, between 2002-2012, for 3 days or longer, were studied. Based on K levels during the hospitalization, the following parameters were calculated: minimal, maximal, range (maximal-minimal) and fluctuation (the gap between two consecutive K levels). The latter parameters were calculated for every K throughout the hospitalization. The associations between the parameters and outcome were assessed using generalized estimating equations model, adjusted to baseline patients’ characteristics and results of other routine laboratory tests (i.e. Sodium, Creatinine and Glucose).
Results: Overall 16,596 admissions of 12,176 patients were included (age 67.8±13.9 years, 66.6% males), and 111,457 K results registered. Overall, patients discharged alive from 15,564 admissions, with an in-hospital mortality rate of 6.2%. Compared with survivors, in-hospital mortalities had higher mean K (4.4±0.8 vs. 4.3±0.6), higher rate of fluctuation or range ≥0.4 (p<0.001 for each). Minimal K throughout the first 48 hours was significantly more prevalent among survivors compared to deceased (41% vs 25% p<0.001). In a multivariate analysis the following parameters were found to be independent prognostic marker for mortality: K<3.9 (adjOR=1.22) or K>4.8 (adjOR=1.17), range ≥0.8 (adjOR=1.53) and minimal K during the first 2 days of admission (adjOR=1.49). Furthermore K fluctuation ≥0.4 was associated with increased mortality within the following 72 hours (adjOR=1.37), (p<0.001 for each).
Conclusions: changes in K, in addition to extreme values throughout an admission of AMI patients are strong prognostic markers of in-hospital mortality. Close monitoring of K in addition to further evaluation of mechanisms and interventions in K are in order.
Imtiaz Ahmed Chaudhry
Armed Forces Institute of Cardiology and National Institute of Heart Disease, Pakistan
Title: Effectiveness of maximum functional capacity (VO2 Max): an assessment tool for preoperative suitability in cardiac surgery. A descriptive cross sectional study from Pakistan
Time : 11:15-11:45

Biography:
Dr Imtiaz Ahmed Chaudhry did his Fellowship in General Surgery in 2004, and later completed his second Fellowship in Cardiac Surgery from College of Physicians and Surgeons, Pakistan in 2011. He completed one year training (IMGSS) in Cardiothoracic Surgery at Queen Elizabeth Hospital Birmingham UK, in 2013.
He is working as a consultant cardiac surgeon at Armed Forces Institute of Cardiology and National Institute of Heart Diseases, Rawalpindi, Pakistan.
He is a member of Research Department, Institutional Ethical Review Board and in charge of Adult Cardiac Surgery Database. He has published more than 10 papers in reputed scientific journals.
Abstract:
Objective: There has been an increase in the number of cardiac surgeries, and there is a growing need to predict the morbidity, mortality and quality of life in patients following such surgery. According to recent studies preoperative identification of patients at risk of postoperative cardiac complications is readily achievable using noninvasive cardiopulmonary exercise testing (CPET). This study evaluated the value of VO2 max testing in the preoperative assessment of patients undergoing elective cardiac surgery and whether poor preoperative cardiopulmonary reserve and comorbid state dictate high risk status and predict complications in patients undergoing elective cardiac surgery.
Methods: A descriptive cross sectional study is being carried out at Armed Forces Institute of Cardiology and National Institute of Heart disease, Rawalpindi, Pakistan. All the patients undergoing elective CABG surgery were included according to inclusion criteria. Data were collected on functional status, postoperative complications, and survival.
Results: Initial analysis revealed a mean age of 52 years ± 10.37 and majority of male patients with a mean BMI of 25.1±. Mean VO2 max at admission was 13.6±4.3 whereas VeO2 and VeCO2 were (46.7±25.4) (30.1±15.72) respectively. Postoperatively our cohort of patients had a mean ICU stay of (54.4 hrs±58.09) and ventilation time of 5.3hrs±4.38. Majority of the patients were weaned off with mild inotropes and only one patient had peroperative IABP insertion. In our study preoperative VO2max cardiopulmonary status positively correlates with postoperative prolonged ICU stay and ventilation time at pearson coefficient r=0.422, r=0.485.
Conclusion: CPET is a useful adjunctive test for predicting postoperative outcome in patients being assessed for cardiac surgery.
Maria Kalliopi Konstantinidou
Royal Brompton and Harefield NHS Trust, UK
Title: TLR-4, CD14 polymorphisms and plasma concentration of Soluble CD14; is there a genetic link with Coronary Artery Disease?
Time : 11:45-12:15

Biography:
Ms Maria Kalliopi Konstantinidou studied at the Medical University of Crete with a Scholarship to Boston University. Subsequently she got involved in research at the University of Athens and completed her PhD, which focused on the genetic predisposition to coronary artery disease, as well as a Masters degree in Thoracic Oncology. Having concluded her cardiothoracic surgery training, in hospitals both in Greece and the UK, she is currently a Clinical Fellow in Cardiothoracic Surgery at Royal Brompton and Harefield NHS Trust in London. Ms Konstantinidou has continued to be active in research co-writing and publishing a number of articles.
Abstract:
Background: Inflammatory mechanisms have a key role in the pathogenesis of atherosclerosis. The most frequent functional polymorphisms of TLR-4- Asp299Gly and Thr399Ile- and of CD14 promoter area - C260T polymorphism- are studied in patients with coronary atheromatosis. Plasma levels of soluble CD14 are checked for possible correlation with the severity of Coronary Artery Disease (CAD).
Methods: DNA was obtained from 100 human paraffin-embedded aortic specimens, from cadavers with known coronary atheromatosis (Group A) and 100 blood samples from patients with CAD, as detected by cardiac Multi-Detector-row-Computed-Tomography (MDCT) (Group B). Our control group consisted of 100 healthy individuals (Group C). Genotyping was performed by Restriction Fragment Length Polymorphism-Polymerase Chain Reaction (RFLP-PCR). Plasma levels of sCD14 were measured with ELISA.
Results: For TLR-4 Asp299Gly and Thr399Ile polymorphisms, no statistically significant differences were observed. Regarding the C260T polymorphism, frequencies of T allele were significantly higher in the control group compared to the case group (p = 0.05). The Odds Ratio (OR) showed statistically significant association of TT genotype with healthy individuals (OR= 0.25, 95% Confidence Interval (CI) = 0.10–0.62, p = 0.0017). Plasma levels of sCD14 in patients with CAD (mean value = 1.35 μg/ml) were reduced when compared to reference value.
Conclusions: The studied polymorphisms of TLR-4 showed no association with CAD. Conversely, the studied functional polymorphism of CD14 has a statistically significant difference in expression between healthy and affected by CAD individuals. Further studies could prove the use of sCD14 as possible biomarker for severe coronary disease.
Interventional Cardiology | Coronary Heart Diseases | Cardiovascular Surgery
Farrah Pervaiz
Armed Forces Institute of Cardiology and National Institute of Heart Disease, Pakistan
Title: Reducing surgical site infections through quality improvement initiative: A tertiary cardiac care facility experience in a developing country
Time : 12:15-12:45

Biography:
Dr Farrah Pervaiz has completed her Masters in Public Health from Quaid e Azam University, Islamabad, Pakistan in 2012. Although, a clinician at genes, possesses a special interest in cardiac research, especially clinical / outcomes based research in order to make everyday medicine more up to date and beneficial to the patients.
She is currently working as Director Research and Development department AFIC/NIHD Rawalpindi. She is the founder member of Research Department and Institutional Ethical Review Board.She is also supervising master thesis and has been a research coordinator for national and international clinical trials. Her Research work is extensively disseminated through more than 50 peer reviewed publications in both National and International Scientific Journals.
Her thesis work has been recently published in British Medical Journal and has been an author of many national publications.
Abstract:
Amongst healthcare associated infections (HAIs), surgical site infections (SSIs) are a preventable cause of increased morbidity and mortality and are associated with substantial financial costs. SSI rates are an indicator of the quality of surgical and postoperative care, which necessitates the need for robust surveillance systems for these healthcare associated infections. Patients undergoing coronary artery bypass grafting (CABG) are at a greater risk for infection due to their relatively older age and the presence of comorbid conditions like diabetes mellitus and obesity.
Objective: To establish the adult cardiothoracic surgical site infections registry to determine adult surgical site infection (SSI) rates and study impact of quality improvement initiatives on SSI rates.
Methods: The Adult Cardiothoracic SSI registry was developed at Armed Forces Institute of Cardiology and National Institute of Heart Disease, Rawalpindi, Pakistan. Monthly SSI rates were monitored for both CABG and valvular heart surgeries inclusive of chest and leg SSIs instituted to control the increased SSI rate in October 2014 after a multidisciplinary approach.
Results: A total number of 1341 cardiac surgeries were carried out and the cumulative SSI rate was 1.7% (n=23) for a period of one year i.e. August 2014 to August 2015, The SSI rate for chest infections was 22% (n=6) and for leg wound (harvest site) infections was 78% (n=17). There was an increase in SSI rate 5% (n= 04) during October 2014. After process improvements the rate declined to 1% in November 2014 and has remained less than or equal to 2% as of August 2015.
Conclusion: A high SSI rate was investigated and multi-modal process improvements and infection control measures were implemented, leading to a decrease in SSI rate from 4% to 1%.
Ahmed Mostafa
Ain Shams University, Egypt
Title: Review of sixty tracheal resections and anastomosis. A seven year experience of a tertiary egyptian referral institute
Time : 12:45-13:15

Biography:
Dr Ahmed MOSTAFA completed his Thoracic Surgery MD in 2009 from Faculty of Medicine- Ain Shams University. He got his pre MD training in France and worked at reputed hospitals such as HEGP-Hôpital Européen Georges-Pompidou, Tenon Hospital. He acquired the MRCS, and he is GMC registered. He has special interest in Airway Surgery. The division of thoracic surgery at Ain Shams University hospitals has quadrupled its annual number of tracheal surgeries since 2009 due to the persistent adoption of the aforementioned management
Abstract:
Introduction: Tracheal stenosis is one of the major complications following prolonged endotracheal intubation. Tracheal resection and anastomosis has proved to be the best solution for this serious problem. This study aims to review the experience of our institute in 7 years with patients presenting with postintubational tracheal stenosis.
Methods: A retrospective study was performed in the period between January 2009 to January 2016. This study involved patients who presented to Ain Shams University Hospitals with postintubational tracheal stenosis, and who underwent tracheal resection and anastomosis as a primary treatment.
Results: We operated upon 60 patients. We excluded glottic stenosis pathology, and patients with major co-morbidities with tracheostomies or stents as definitive treatment . Patients included 42 males (70%), 18 females (30%). Mean age was 28.35 (ranging from 2 to 72 years). At presentation, 45 patients ( 70%) had previous endoscopic dilataions, 38 patients (63.3%) had tracheostomies, 19 patients ( 31.6%) had history of tracheal stenting. Seventeen patients (28.3%) had cricotracheal resections (CTR) for subglottic stenosis. Cervicotomy was sufficient in 41 patients (68.3%), additional manubriotomy was needed in 15 patients (25%), while full sternotomy was done in only 4 patients (6.6%). All patients were given a chance for immediate postoperative extubtion. Anastomotic success rate was (96.6%). In hospital mortality was (1.6%).
Conclusion: Tracheal resection and anastomosis proves to be a safe and satisfactory option for postintubational tracheal stenosis. This intervention must be applied widely in developmental countries where there is frequent rush for tracheostomies, and abuse of tracheal stenting and dilatation. Quality of life improves dramatically following an effective surgery.

Biography:
She has completed her Medical degree (Professional Doctorate) at the age of 26 years from Guilan University of Medical Sciences. She has 5 published and 3 under publish articles. She is the reviewer of the Journal of Biology and Today`s World (An International Biomedical Journal).
Abstract:
Background: Nowadays, percutaneous coronary intervention (PCI) is the most commonly used nonsurgical procedure which restores blood flow to the heart tissue. Such procedures may stimulate myocardial injury and release of myocardial necrosis biomarkers. Although higher levels of cardiac troponins (cTns) are associated with later adverse events, the prognostic importance of the lower levels of cTns, especially highly sensitive assays, is still a matter of controversy.
According to the above points, in the present study, we aimed to assess the prognostic power of mild to moderate elevations in hs-cTnT levels (as an indicator of periprocedural myocardial necrosis) for predicting the one-year outcome of PCI.
Methods and Results: In the present study, all the patients undergoing elective PCI between March 2011 and April 2013 at Tehran Heart Center were followed up. Based on our inclusion and exclusion criteria, finally, 2309 patients were qualified for the study. For measuring hs-cTnT, three blood samples were drawn: the first immediately before the beginning of PCI (baseline), the second 6 h after PCI, and the last 12 h after PCI. The hs-cTnT levels were analyzed using Elecsys 2010 analyzer and major adverse cardiac events (MACE) were assessed one month and one year after the procedure. Based on the pre- and post-procedural hs-cTnT levels, the patients were divided into three groups. But, the differences between the three hs-cTnT groups in terms of frequencies of MACE were not significant.
Conclusions: This prospective study demonstrated no association between mild to moderate elevations in hs-cTnT after PCI and one-year MACE.
Adel Kamel Abdel Malek
Assiut University, Egypt
Title: Implication of protein restriction on the developing heart of albino rat
Biography:
To be updated soon...
Abstract:
Background: Protein malnutrition has become an alarming problem in developing countries and refugee camps.
Aim of the work: The present work aims at studying the effects of maternal protein malnutrition on the structure of the heart of their off-springs.
Material and methods: 20 adult female albino rats were divided into two groups; the first group was fed normal protein diet contained 20% casein and considered as control. The second group were fed low protein diet with 9% casein and considered the experimental group. All breeder rats were habituated to their respective diets for two weeks before mating, during pregnancy and lactation. Hearts of the pups were examined at birth and at the age of one month.
Results: Hearts of pups of undernourished mothers showed cardiac myocytes with fractures of and cytoplasmic vacuulations. There was mitochondrial swellings and dehescience of the intercalated discs.
Conclusion: Changes in the structure of cardiac muscle fibers as a result of protein undernutrition is a potential insult that might lead to irreversible derangement in contractile functions of the heart.
Nattapong Thaiyanurak
Siriraj Hospital, Thailand
Title: Prevalence of anatomical aortic arch variants in Thai patients undergoing thoracic aorta computed tomography angiogram
Time : 14:45-15:15

Biography:
Dr. Nattapong Thaiyanurak graduated his MD from College of Medicine, Rangsit University, Bangkok. He completed his residency in internal medicine and cardiology fellowship training from Siriraj Hospital, Mahidol Universtiy, Bangkok. He is currently the cardiologist at the Lampang Hospital and devotes his time in teaching medical students of Lampang Hospital Medical Education Center, Chiang Mai University.
Abstract:
Yanal F. Al-Naser
Queen Alia Heart Institute, Jordan
Title: 35 years off warfarin-Standing the “Test “or “Challenge†of time?
Time : 15:15-15:45
Biography:
Yanal Al-Naser is a consultant cardiac surgeon from Amman-Jordan. He graduated from University of Jordan in 1999 and was awarded the Jordanian boards in general surgery (2004) and cardiac surgery (2009). He was trained in Manchester –England as an adult cardiac surgeon and finished his training in 2012. He became a consultant adult cardiac surgeon in 2012 at Queen Alia Heart Institute in Jordan. He has a number of publications, and is a member of the Jordanian Cardiac society and the Royal College of Surgeons in the UK.
Abstract:
A 46 year old female patient, with no medical illnesses was referred to my clinic with effort intolerance and palpitations of four years duration. Her history dates back to when she was 11 when she had an Aortic and Mitral valve replacement due to rheumatic causes, she had a size 19mm bileaflet mechanical aortic valve and a size 27mm bileaflet mechanical mitral valve. She was started on warfarin and took it for three months of her life as documented by her family members and follow up notes till she decided to stop it. She stated that she took no medications at all and was completely asymptomatic, she got married and had three children, all a normal vaginal delivery aided by a mid wife at home. Her 2DECHO showed a grade three para-leaking aortic and mitral valves, and was referred to me for a redo AVR and MVR 35 years later, being off warfarin for all that period and was asymptomatic for 30 years and never had a stuck valve. Her coagulation profile was normal, with an INR of 1, I operated on her and found a rim of pannus surrounding the valves, but the leaflets were mobile. I replaced both valves using St Jude size 21 Aortic Valve and size 29 Mitral valves, both mechanical. There are a few cases described in literature about mechanical valves with no warfarin, but I believe this is one of those with the longest –off warfarin- history.
Elisabet Berastegui
Hospital Universitari Germans Trias i Pujol, Spain
Title: Creating a new and simply frailty score for predicting postoperative morbidity in cardiac surgery
Time : 15:45-16:15

Biography:
Elisabet Berastegui completed her studies of Medicine in Barcelona University- Hospital Clinic. She completed her training in Cardiac Surgery in Hospital Vall Hebron where she got her Certificate of research aptitude: Fallot Tetralogy ; Right ventricular remodelling after pulmonary valve replacement in 2010. She works like staff in Hospital Germans Trias I Pujol where is working in areas of frailty and risk, ( Doctoral Programm. Development of Thesis in Autonoma Barcelona University. She is enrolled in differente studys ( PERSIST TRIAL ) and is Coordinator of Spanish PLIAR REGISTER, ( for sutureless prosthesis)
Abstract:
Ageing and elderly people have greater risk. Physical state and frailty status represent an important risk and must be considered before cardiac surgery. More than one third of current surgeries are performed in patients older than 70 years; This is a factor to keep on mind in our routine evaluation. Currently an accepted definition for frailty is not well established. It has been considered as a physiological decline in multiple organ systems, decreasing the patient’s capacity to withstand the stresses of surgery and disease. The aim of our study was to determinate a correlation between preoperative features and the morbidity after cardiac surgery in aortic valve replacement population.
Methods. We selected the 70 years old patients or older who underwent an elective aortic valve replacement. We collected prospectively all preoperative features and frailty traits (Barthel Test; Gait Speed test, Handgrip) also taking into account blood parameters like albumin level and hematocrit previous to the surgery, hospital admissions within 6 months, and we analyze the demographics and medical history of the patients. We compare patients who undergo to stented prosthesis, sutureless or TAVI procedure.
Image
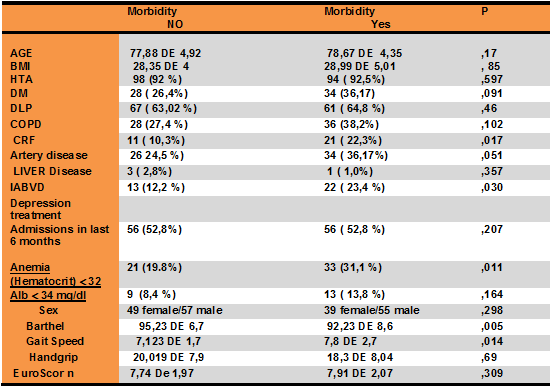
(BMI body mass index, HTA hypertension, DM diabetes mellitus, COPD Pulmonary obstructive disease, IRC chronic renal failure, DLP dyslipidemia, IADL Independence activities daily living)
Results: Two hundred patients were enrolled. The mean age was 78 years all. The predicted mortality with Logistic euroScore I was 12,8% with a real mortality lower than expected (3,5%). Pre-surgery frailty in our population was associated with a Gait Speed higher of 7 seconds, Barthel less of 90%, anemia with Hematocrit <32%, albumin level< 3,4g/dl, chronic renal failure, preoperative re-admission and artery disease. The TAVI group had higher morbidity, no differences statistically significant between Stented and sutureless prosthesis group. Frail individuals had longer hospital stays, readmissions and respiratory/ infectious complications. The mortality at 6 months /one year follow up was 4,1 % /0 % respectively; and morbidity ( pacemaker implant, respiratory events, readmission); at 6 months /one year of follow up was 13,47 % to 3%.
Conclusions: Elderly and frailty population present more complications after a cardiac surgery. A simple frailty score must be considered in cardiac population to avoid increased morbidity.
Poster Presentations 16:30-17:30
Ersöz Gonca
1Bulent Ecevit University, Turkey
Title: A pharmacological study of a new spiro-cyclic benzopyran activator of the cardiac mitoKATP channel on ischemia/reperfusion-induced ventricular arrhythmias

Biography:
Ersöz Gonca has completed his PhD in 2008 from Abant Ä°zzet Baysal University and Post-doctoral studies from Robert Gordon University, the Institute of Health and Welfare Research in 2012. He is studying ischemia/reperfusion-induced ventricular arrhythmias and myocardial injury. He has been conducting his researches in Bülent Ecevit University, Biology Department since 2009.
Abstract:
Background/Introduction: 4’-(N-(4-acetamidobenzyl))-2,2-dimethyl-2,3-dihydro-5’H-spiro [chromene-4,2’-[1,4]oxazinan]-5’-one (compound A) was synthesized as a new spiro-cyclic benzopyran activator of the cardiac mitochondrial ATP-dependent potassium (mitoKATP) channels. A previous study showed the anti-ischemic properties of Compound A.
Purpose: This study was performed to research the effect compound A on ischemia/reperfusion (I/R)-induced ventricular arrhythmias. In our previous study, we suggest that both mitoKATP channel activation and sarcolemmal ATP-dependent potassium (sarcKATP) channel inhibition confer protection against I/R-induced arrhythmias; therefore, we also aimed to test the hypothesis that a combination of mitoKATP channel activation and sarcKATP channel inhibition may be even more effective at decreasing ventricular arrhythmias.
Methods: We performed myocardial I/R by ligating the left main coronary artery for 6 minutes followed by loosening the bond at the coronary artery for 6 minutes in anesthetized rats. The experimental groups were as follows: (1) Vehicle control, (2) Compound A (3 mg/kg) (3) Compound A (10 mg/kg.) (4) Diazoxide (5) HMR 1098 (6) Compound A (10 mg/kg)+HMR 1098 and (7) Diazoxide+HMR 1098 group.
Results: Compoud A at a dose of 10 mg/kg decreased both the arrhythmia score and the total length of arrhythmias (P<0.01). Diazoxide at a dose of 40 mg/kg, a selective mitoKATP channel opener as a reference drug only decreased the total length of arrhythmias (P<0.01). Compound A at a dose of 10 mg/kg was more effective at decreasing the duration of arrhythmias than a dose of 3 mg/kg of compound A and diazoxide. The combination of both diazoxide and compound A with HMR 1098, a selective sarcKATP channel blocker, did not exhibit any additive or synergic effect on the antiarrhythmic effect of each drug alone.
Conclusion(s): These results reveal that compound A may have a dose-dependent antiarrythmic effect, which is more pronounced than the antiarrhythmic effect of diazoxide. Both mitoKATP channel activation and sarcKATP channel inhibition at the same time may not reveal any additive antiarrhythmic effect on I/R-induced arrhythmias.
Anton Cherepov
Federal Research Clinical Center, Russia
Title: Possible mechanisms of peripheral blood pressure adaptation to simulated chronic hypogravity

Biography:
Mr. Anton Cherepov graduated from Medical-Biology Faculty (Biochemistry department) of N.I.Pirogov Moscow Medical Institute in 1989. His first research dealt with the role of lipid peroxidation in Parkinson diseases at the Institute of General Pathology and Pathophysiology, Russian Academy of Medical Sciences. Then he studied immediately-early genes expression in learning and memory on the model of filial imprinting in chicks and other learning models in mice at P.K.Anokhin Institute of Normal Physiology, Russian Academy of Medical Sciences. His current research interest involves methodological approaches for evaluation of specific and non-specific responses of human organism under normal and extreme conditions
Abstract:
Human adaptation to extreme conditions primarily involves the basic vital systems of the body. The aim of our study was to analyze the mechanisms of adaptation of the cardiovascular system to simulated conditions of space flight and stay on the lunar surface.
Hypo- and microgravity was simulated using orthostatic and antiorthostatic hypokinesia, respectively (bedrest at different angles: -6° and +9.6°) and was carried out on volunteers in hospital setting.
Analysis of blood pressure variability (BPV) revealed significant increase in the systolic BPV by 8 day in head-down bedrest group (HDBRG) and return of these parameters to baseline values by day 21. Analysis of the frequency components of systolic BPV spectrum in HDBRG showed that the main contribution to the total spectral power on day 8 was made by the very-low-frequency component. At the same term, we observed a pronounced increase in the very-low-frequency component of heart rate variability (HRV) in HDBRG in comparison with that in head-up bedrest group (HUBRG). Coincidence of these changes may indicate that significant contribution into adaptation is made by central neural mechanisms that are activated during the first week of simulated microgravity. The diastolic BPV was markedly changes by day 21 in both experimental groups in comparison with baseline values, primarily at the expense of very-low-frequency component of BPV. In HRV, no similar changes were observed by day 21 of the experiment. These findings probably attest to predominance of local mechanisms of vascular tone regulation not directly related with the autonomic control.
Riccardo Turri
Mirano General Hospital, Italy
Title: Multi-district atherosclerotic disease: mid-term outcome of hybrid or totally endovascular coronary and carotid revascularization

Biography:
Riccardo Turri graduated with the best ratings at Padua University in Italy; he was always engaged in studying and applying into invasive cardiology and acute cardiologic care. His competences include coronary angioplasty, bifurcation lesions, coronary imaging and functional assessment, limb and BTK angioplasty. In the last 3 years he worked as an interventional cardiologist at Mirano General Hospital, near Venice, in Italy.
Abstract:
Background: The socio-economic impact of multi-district atherosclerotic disease is elevated for frequent hospitalizations and morbidity/mortality.
Aim: Assess clinical characteristics, angiographic findings, therapeutic strategy and outcome of patients hospitalized with a concomitant diagnosis of coronary artery and carotid obstructive diseases.
Methods: We evaluate all patients hospitalized from 2006 to 2012. Revascularization strategies were hybrid (carotid stenting CAS and cardiac surgery CABG) or totally endovascular (coronary angioplasty PCI and CAS).
Results: 107 patients enrolled, 42.1% hospitalized for carotid obstructive disease (groupA), 57.9% for coronary artery disease (groupB). Patients were treated with PCI and staged CAS in 28% of cases (15.6% in groupA, 37.1% in groupB), with CAS and staged PCI in 21.5% of cases (46.7% in groupA, 3.2% in groupB), with CAS and simultaneous CABG in 39.3% of cases (24.4% in groupA, 50% in groupB) and with PCI and simultaneous CAS in 11.2% of cases (13.3% in groupA, 9.7% in groupB). 30-days results: mortality 0%, major/minor stroke 3.7% (2.2% in groupA, 4.8% in groupB), myocardial infarction 2.8% (0% in groupA, 4.8% in groupB), major bleeding 5.6% (2.2% in groupA, 8.1% in groupB). Major bleeding affected only patients with acute symptoms and 11.9% of patients following CABG. Follow-up results: cardiovascular mortality 4.7% (2.2% in groupA, 6.5% in groupB), all-cause mortality 2.8% (4.4% in groupA, 1.6% in groupB), stroke 0.9% (2.2% in groupA, 0% in groupB), myocardial infarction 2.8% (4.4% in groupA, 1.6% in groupB). The only predictor of mortality at follow-up was the inhospital stroke (HR 7.6 for all-cause mortality, 16.5 for cardiovascular mortality).
Conclusions: Patients with concomitant coronary artery disease and carotid obstructive disease were treated with a high procedural success, following a hybrid or totally endovascular revascularization. Patients hospitalized in an acute setting have more strokes and bleedings at 30 days; these patients need therefore most careful assessment and treatment.
Rawa Delshad
Hawler Medical University, Iraq
Title: Utility of cardiac biomarkers in combination with exercise stress testing in patients with suspected ischemic heart disease
Biography:
To be updated soon...
Abstract:
Eighty patients with suspected ischemic heart disease were enrolled in the present study. They were classified into two groups: patients with positive exercise stress test results (n=40) and control group with negative exercise stress test results (n=40). Serum concentration of troponin I, Heart-type Fatty Acid Binding Protein (H-FABP) and Ischemia Modified Albumin (IMA) were measured one hour after performing stress test. Enzyme Linked Immuno-sorbent Assay was used to measure both troponin I, H-FABP levels, while IMA levels were measured by albumin cobalt binding test. There was no statistically significant difference in the mean concentration of troponin I between two groups (0.75±0.55ng/ml) for patients with positive test result vs. (0.71±0.55ng/ml) for negative test result group with P>0.05. Contrary to our expectation, mean IMA level was slightly higher among control group (70.88±39.76U/ml) compared to (62.7±51.9U/ml) in positive test result group, but still with no statistically significant difference (P>0.05). Median H-FABP level was also higher among negative exercise stress testing group compared the positive one (2ng/ml vs. 1.9ng/ml respectively), but failed to reach statistically significant difference (P>0.05). When quartiles model used to explores the possible association between each study biomarkers with the others; serum H-FABP level was lowest (1.7ng/ml) in highest quartile of IMA and lowest H-FABP (1.8ng/ml) in highest quartile of troponin I but with no statistically significant association (P>0.05). Myocardial ischemia, more likely occurred after exercise stress test, is not capable of causing troponin I release. Furthermore, an increase in H-FABP and IMA levels after stress test are not reflecting myocardial ischemia. Moreover, the combination of troponin I, H-FABP and IMA after measuring their post exercise levels does not improve the diagnostic utility of exercise stress test enormously.
Khizar Khan-Mahmood
Colchester General Hospital, Colchester, Essex, UK
Title: The root of all evil: A case reeport documenting the presentation of an aortic root abscess in a 26 year old gentelman

Biography:
Dr Khan-Mahmood completed his MBBS age 24 from Barts and the London School of Medicine and Dentistry, Queen Mary University of London. During this time, he intercalated in Oral Biology, and gained a BSc (first class honours). He graduated with a MBBS and BSc (hons). Dr Khan-Mahmood went on to complete foundation training at Addenbrookes Hospital, Cambridge University Trust. He took a year out of training, to set up various business ventures and to travel, volunteering in health services around the world. Currently a Core Medical Trainee at Colchester General Hospital, Essex, with a keen specialist interest in Cardiology.
Abstract:
Background: Aortic root abscesses are a complication of infective endocarditis. A devastating disease with high morbidity and mortality leading to complications such as atrioventricular septal destruction, even death.
Objectives
Demonstrate importance of coordination between health professionals.
Highlight importance of examination, investigation and senior support.
Demonstrate how young patients maintain good physiological reserve masking severe infection.
Materials and Methods:Literature search. Patient consented.
Results: TTE demonstrated normal left ventricular function, EF 50-55%, and an unusual aortic valve anatomy with significant aortic regurgitation.
Blood cultures were negative; IV amoxicillin and IV gentamycin were commenced.
TOE revealed thickened aortic leaflets and moderate aortic regurgitation, suggesting infective endocarditis. Aortic root was suspicious of an aortic root abscess.
Patient continued to spike temperatures. Antibiotics changed to gentamycin, vancomycin and rifampicin. Case discussed at cardiothoracic centre. Patient was diagnosed with aortic root abscess, transferred and underwent an aortic root and mechanical valve replacement.
Specimen was culture negative, PCR positive for Staphylococcus lugdunensis. Post-operatively commenced on warfarin and a four month course of rifampicin and daptomycin.
Conclusions: Young patients mask a multitude of sins and present with subtle symptoms given good physiological reserve. The root of all evil was the aortic root.
Clear, precise, detailed history and review of results highlights serious cases early, benefitting from prompt review.
Aortic root abscess is a serious complication of infective endocarditis and should always be considered if symptoms do not respond to treatment after 72hrs.
Specialist input is useful and important. Advances in cardiac imaging allows useful investigative correlation, with the ultimate treatment option being cardiothoracic surgery.
Ygal Plakht
Ben-Gurion University of the Negev, Israel
Title: Acute myocardial infarction: The association of changes in K+ levels and in-hospital mortality of patients with acute myocardial infarction
Biography:
To be updated soon...
Abstract:
Background: serum potassium levels (K, mEq/L) of patients with acute myocardial infarction (AMI) were found to be associated with short- and long-term outcomes. Nevertheless, significant fluctuations in K have been reported during the acute phase of an AMI.
Aims: to evaluate the association between K changes during the hospitalization and in-hospital mortality of patients admitted with AMI.
Methods: AMI patients hospitalized in a tertiary medical center, between 2002-2012, for 3 days or longer, were studied. Based on K levels during the hospitalization, the following parameters were calculated: minimal, maximal, range (maximal-minimal) and fluctuation (the gap between two consecutive K levels). The latter parameters were calculated for every K throughout the hospitalization. The associations between the parameters and outcome were assessed using generalized estimating equations model, adjusted to baseline patients’ characteristics and results of other routine laboratory tests (i.e. Sodium, Creatinine and Glucose).
Results: overall 16,596 admissions of 12,176 patients were included (age 67.8±13.9 years, 66.6% males), and 111,457 K results registered. Overall, patients discharged alive from 15,564 admissions, with an in-hospital mortality rate of 6.2%. Compared with survivors, in-hospital mortalities had higher mean K (4.4±0.8 vs. 4.3±0.6), higher rate of fluctuation or range ≥0.4 (p<0.001 for each). Minimal K throughout the first 48 hours was significantly more prevalent among survivors compared to deceased (41% vs 25% p<0.001). In a multivariate analysis the following parameters were found to be independent prognostic marker for mortality: K<3.9 (adjOR=1.22) or K>4.8 (adjOR=1.17), range ≥0.8 (adjOR=1.53) and minimal K during the first 2 days of admission (adjOR=1.49). Furthermore K fluctuation ≥0.4 was associated with increased mortality within the following 72 hours (adjOR=1.37), (p<0.001 for each).
Conclusions: changes in K, in addition to extreme values throughout an admission of AMI patients are strong prognostic markers of in-hospital mortality. Close monitoring of K in addition to further evaluation of mechanisms and interventions in K are in order.
Abdullah Nabi Aslan
Ankara Ataturk Education and Research Hospital, Turkey
Title: Coexistence of gitelman syndrome and hypertrophic obstructive cardiomyopathy in a pregnant woman

Biography:
Abdullah Nabi ASLAN has completed his PhD at the age of 25 years from Marmara University and postdoctoral studies from Ankara Ataturk Education and Research Hospital,Department of Cardiology. He is a specialist of cardiology. He has published more than 30 papers in reputed journals and has been serving as an editorial board member of Clinical Cardiology Updates journal. I also take a role of reviewer in some reputed journals and like my job too much.
Abstract:
A 34-year-old woman with GS presented at 20 weeks gestation with the complaints of palpitation, fatigue and presyncope. This was her first pregnancy. Her initial diagnosis of GS had been confirmed 4 years ago based on clinical presentation and laboratory data. She was maintained on oral electrolyte replacement with oral potassium chloride and magnesium citrate were prescribed and the course of the pregnancy. At physical examination there was a grade 3/6 systolic ejection murmur maximally heard at apical focus of the heart. Blood pressure was 80/50 mmHg and laboratory test showed a serum potassium value of 2.5 mmol/L (normal 3.5-5.1), a serum calcium value of 10.2 mg/dL (normal 8.6-10.0) and a serum magnesium level of 1.4 mg/dL (1.6-2.6) were noted. Blood gas analysis showed metabolic alcalosis with a pH of 7.495 (normal 7.380-7.460), pCO2 of 35.6 (normal 32-46) and HCO3 of 34.1 mmol/L (normal 22-26). Serum creatinine, urea and remainder ionograms were normal. Electrocardiogram (ECG) showed normal sinus rhythm with a rate of 67 beats per minutes and remarkable ST-T changes at inferior and precordial derivations. There was also a prolonged QT interval (490 ms) (Fig 1). Echocardiography determined a hypertrophic obstructive cardiomyopathy (HOCM) with a septal thickness of 2.1 cm and posterior wall thickness of 1.1 cm (Fig.2a) and a resting gradient of 30 mmHg (Fig. 2b). There was also systolic anterior motion in mitral valve creating a mild degree of mitral regurgitation (video). Risk of SCD at 5 years was calculated as 2.93%. Because the patient was pregnant, the cardiology, gynecology and pediatric departments organised a council whether the patient will maintain the pregnancy or not. The common consensus was close follow-up and if needed termination. At follow-ups, the pregnancy was continued without any complication with a born healhy daughter.
Muhammad Asad Sheikh
Peterborough City Hospital, UK
Title: Cortical blindness post coronary angiogram, a rare but frightening complication

Biography:
Dr. Muhammad Asad Sheikh has completed MBBS degree form Allama Iqbal Medical College, Pakistan and has been in training in UK for last 5 years. He has speacial interest in Cardiology and has done many presentations and teachings on various topics in cardiology.
Abstract:
Cortical blindness is a rare but frightening complication following coronary angiogram probably due to contrast penetration in occipital lobes in susceptible individuals.
A case report of 82 years old man was admitted with collapse. Investigations showed NSTEMI with T wave inversion in lateral leads and Troponin rise. Severe LCX disease was found on coronary angiogram, which was stented with DES with good angiographic results. Patient became blind 30 minutes after the procedure.
Clinical examination showed diminished visual acuity to light perception bilaterally. Light reflex and fundoscopy was unremarkable. Motor, sensory & cerebellar systems were normal. No other abnormality was detected.
CT head scan showed bilateral contrast enhancement in the occipital lobes. Patient was not considered for thrombolysis due to symmetrical bilateral focal neurological presentation, which is uncommon in cerebrovascular accidents. Patient had a partial recovery of vision while in observation ward and had complete recovery within 24 hours. Patient remained asymptomatic at 2 months follow-up post discharge.
A clinical diagnosis of “cortical blindness” was made, however it was thought to be unlikely due to thrombo-embolism secondary to cardiac catheterization so thrombolysis was withheld (symmetrical bilateral focal neurological lesions are very uncommon in cerebrovascular accidents).
A quick literature search showed case reports of cortical blindness linked with coronary angiography and such blindness almost always spontaneously recovers in hours to days time.
Although the exact cause is unknown it is postulated that there is a direct neurotoxic effect of contrast in occipital cortex potentiated by prolonged lying position during coronary angiogram.
Other possible mechanisms includes spasm of the posterior cerebral arteries, dissection of the aortic arch, and contrast-induced hypotension.
Abdullah Nabi Aslan
Ankara Ataturk Education and Research Hospital, Turkey
Title: Impact of coronary artery dominance on P wave dispersion

Biography:
Abdullah Nabi ASLAN has completed his PhD at the age of 25 years from Marmara University and postdoctoral studies from Ankara Ataturk Education and Research Hospital,Department of Cardiology. He is a specialist of cardiology. He has published more than 30 papers in reputed journals and has been serving as an editorial board member of Clinical Cardiology Updates journal. I also take a role of reviewer in some reputed journals and like my job too much.
Abstract:
Background: P-wave duration and dispersion has been proposed as being useful for the prediction of paroxysmal atrial fibrillation (AF). The aim of this study was to investigate the effect of coronary artery dominance on P wave duration and dispersion.
Design and Methods: The study population included 194 patients with left dominant (LD) circulation and 200 age and gender-matched controls with right dominant (RD) circulation and without coronary artery dissease based on invasive coronary angiography findings. The electrocardiogram of each patients was obtained upon admission to hospital and evaluated by two cardiologists blinded to the angiographic results of the patient. P-wave dispersion (PWD) was defined as the difference between the maximum and minimum P-wave duration. Statsitical analyses were performed using SPSS v17.0 statistical software package.
Results: PWD was shown to be significantly prolonged in patients with LD circulation compared to controls with RD circulation (48 ± 14 ms vs 33 ± 15 ms, p = 0.001). P wave duration was similar between the groups (p = 0.124). Moreover, there was positive correlation between PWD and age (r: 0.502, p= 0.009), left ventricular (LV) mass (r: 0.614, p= 0.001), LV mass index (r: 0.727, p< 0.001) and left atrium (LA) diameter (r: 0.558, p= 0.003) in LD circulation patients. Multivariate logistic regression analysis determined age, LV mass index, LA diameter and LD circulation as independent predictors of prolonged PWD.
Conclusions: LD circulation could lead to an increased risk of AF through prolonged PWD. We recommend follow-up of these patients to assess the development of AF in the future.
Nadeeja Himanthi Gamalath Seneviratne
The National Hospital of Sri Lanka, Sri Lanka
Title: Factors associated with survival of post Coronary Artery Bypass Graft (CABG) patients registered in cardiology Unit, National Hospital Sri Lanka (NHSL)

Biography:
Dr. (Mrs) NHG Seneviratne, MBBS (Sri Lanka), MD Medicine (Colombo). – She obtained MD Medicine from Post Graduate Institute of Medicine, University of Colombo in 2013. Currently she is undergoing post doctoral training in Cardiology at Institute of Cardiology NHSL. She has published four papers in local forums and one poster presentation which won the gold medal for best poster in 2010. She has done oral and poster case presentations at Asian Interventional Cardiovascular Therapeutices Congress 2015, Dhaka, Bangladesh. She works as a sub inspector in ODYSSEY and TRIUMPH multi centre clinical trails and a resource person in frailty study.
Abstract:
CABG is one of the treatment options for the patients with coronary artery disease (CAD). This study was aimed to describe survival up to occurrence of cardiac events and factors associated with them among CABG patients at NHSL.
Retrospective analytical study was carried out among the patients who had undergone CABG at least one year before the date of data collection. Cardiac event was defined as new occurrence of any condition namely; unstable angina (UA), ST elevated myocardial infarction (STEMI), non ST elevated myocardial infarction (NSTEMI) and heart failure (HF). Survival was assessed up to the defined cardiac events.
The sample (n=421) consists 74.6% males and mean age was 63.16years (SD = 7.86). Event rates were UA (13.3%), STEMI (0.5%), NSTEMI (3.1%) and heart failure (8.6%). Kaplan-Mayer survival analysis revealed the probability of survival at 5 years was 79.6% (CI 0.781-0.871) and 10 year was 58.1% (CI 0.516- 0.688). Cox regression revealed significant associations with age (HR- 0.973, p=0.023), family history (FH) of hypertension (HR-2.2, p=0.044) compared to negative family history and activities of daily living (ADL) independency (HR=0.16, p= 0.011) compared to the ADL dependency.
CABG surgery reserves its own place in management of CAD. Sri Lankan survival data of CABG patients seems to be similar to other countries of the world. Age, status of ADL prior to CABG and family history of hypertension were significantly associated with survival.
Withma Muthukumara
Lancaster Medical School, UK
Title: Case-based evaluation of the effectiveness of PCI and CABG in the management of multi-vessel Coronary Artery Disease
Biography:
To be updated soon...
Abstract:
Introduction: Multi-vessel coronary artery disease (CAD) can give rise to numerous disabling symptoms such as angina, shortness of breath (SOB) and fatigue, considerably impairing quality of life (QoL). Percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) have been developed to overcome these and increase life expectancy. The controversy over treatment preference has been a historical battle which CABG has dominated. However, the development of drug eluting stents (DES) is reducing the margin of difference in symptom improvement between the two interventions, making decisions difficult. Large randomized control trials (RCTs) such as SYNTAX, ARTSI/II and FREEDOM have set out to investigate the outcomes for each treatment and provide recommendations.
Aims: To measure QoL in terms of the symptom experience between 4 patients who had PCI/CABG and recognise the intervention providing the largest relief of symptoms. Additionally, explore the evidence behind PCI and CABG for multi-vessel CAD from RCTs and compare their outcomes with Case findings.
Method: 4 clinical cases, 2 undergoing PCI and 2 undergoing CABG, with multi-vessel CAD were selected. QoL was assessed using the Cardiovascular Limitations And Symptoms Profile (CLASP) questionnaire to explore the severity of symptoms before and after the intervention.
Results: Patients in the PCI group had an overall symptom reduction of 57.9% compared to only 38.9% in the CABG group. The greatest effect was seen in the angina category for PCI and SOB category for CABG, which resulted in a 100% relief of symptoms.
Conclusion: All patients had an improvement in symptoms to some degree, regardless of the type of intervention, but PCI patients had better outcomes across 4 more categories than CABG patients. RCTs report greater relief of symptoms following CABG, which was inconsistent with Case findings. CABG has demonstrated an increase in life expectancy and QoL in patients with SYNTAX scores ≥23 and more severe multi-vessel CAD, especially in diabetic patients, making it the treatment of choice.